Enhance your health with free online physiotherapy exercise lessons and videos about various disease and health condition
CONUS MEDULLARIS AND CAUDA EQUINA INJURIES
The conus medullaris, which is the terminal segment of the adult spinal cord, lies at the inferior aspect of the L1 vertebrae. The segment above the conus is termed the epiconus, consisting of spinal cord segments L4-S1. Lesions of the epiconus will affect the lower lumbar roots supplying muscles of the lower part of the leg and foot, with sparing of reflex function of sacral segments. The bulbocavernosus reflex (i.e., reflex contraction of the anal sphincter in response to compression of the glans penis or clitoris) and micturition reflexes are preserved, representing an upper motor neuron (UMN) or suprasacral lesion. Spasticity will most likely develop in sacral innervated segments (toe flexors, ankle plantarflexors, and hamstring muscles). Recovery is similar to other UMN SCIs.
Conus Medullaris lesions
Conus lesions affecting neural segments S2 and below will present with lower motor neuron (LMN) deficits of the anal sphincter and bladder due to damage of the anterior horn cells of S2-S4. Bladder and rectal reflexes are diminished or absent, depending on the exact level and extent of the lesion. Motor strength in the legs and feet may remain intact if the nerve roots (L3-S2) are not affected.
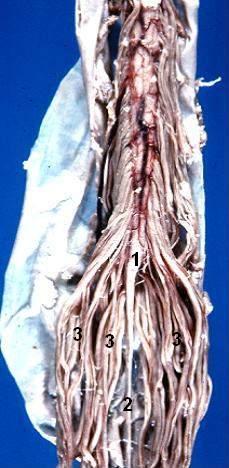
Human caudal spinal chord - Anterior view
- 1) Conus medullaris
- 2) Filum terminale
- 3) Cauda equina
Cauda Equina lesions
Read more about this Syndrome in Wikipedia Here- wiki
Injuries below the L1 vertebral level usually affect the cauda equina or nerve rootlets supplying the lumbar and sacral segments producing motor weakness and atrophy of the lower extremities (L2-S2) with bowel and bladder involvement (S2-S4), and areflexia of the ankle and plantar reflexes. Often the patient may have spared sensation in the perineum or lower extremities, but still have paralysis. In cauda equina injuries there is loss of anal and bulbovernosus reflexes, as well as impotence. Cauda equina injuries have a better prognosis for recovery most likely due to the fact that the nerve roots are more resilient to injury. Cauda equina injuries may represent a neuropraxia or axonotmesis and demonstrate progressive recovery over a course of weeks and months. As the cauda equina rootlets are histologically peripheral nerves, regeneration can occur.
Separation of cauda equina and conus lesions in clinical practice is difficult, because some of the clinical features of these lesions overlap. Pain is uncommon in conus lesions but is frequently a complaint in cauda equina lesions. Sensory abnormalities occur in a saddle distribution in conus lesions and, if there is sparing, there is usually dissociated loss with a greater loss of pain and temperature while sparing touch sensation. In cauda equina lesions, sensory loss occurs more in a root distribution and is not dissociated.
Return From conus medullaris to Home Page
SCI Related Pages







Recent Articles
|
Author's Pick
Rating: 4.4 Votes: 252 |


 About Prodyut Das (PT, DPT) Physical Therapist at SMC, New York, USA. Former PT Winner Regional Health, South Dakota, Former HOD Physiotherapy & Fitness center @ NIMT Hospital, Greater Noida. Former PT ISIC Hospital. DPT ( Univ of Montana), MPT (neuro), MIAP, cert. manual therapist, Medical Neuroscience (USA). Licensed Physical Therapist in NY and Texas, USA. |
Connect with me- |
© Copyright physiotherapy-treatment.com since 2009 |