Enhance your health with free online physiotherapy exercise lessons and videos about various disease and health condition
Brown Sequard Syndrome
Brown Sequard Syndrome results from a transverse hemisection of the spinal cord, whereby half of the spinal cord is damaged laterally (Sullivan 1989).
Cause Lateral damage to one side of the cord may be caused by penetration injuries such as stab wounds but may also result from other etiologies and injury mechanisms such as road traffic accidents and rugby football injuries. Fracture dislocation of a unilateral articular process and acute ruptured inter vertebral disc have also been reported to give rise to this syndrome (Sullivan 1989).
Although knife injuries may result in the classical picture of Brown-Sequard syndrome, they are relatively uncommon. In over 1600 cases of spinal cord injury in America, only 1.1% were due to penetrating injuries other than gunshot wounds (Waters et al 1995). However, in South Africa, of 1600 patients admitted to a spinal injuries unit, a quarter were the result of stab wounds. Of these, 50% had the Syndrome (Peacock et al 1977).
Clinical Picture of Brown Sequard Syndrome
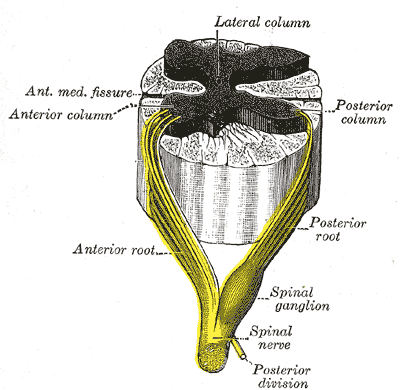
Motor deficit. Motor loss occurs on the same side as the lesion due to destruction of the pyramidal tracts. The lower motor lesion, resulting from damage to the anterior horn cells at the level of the lesion, will be particularly significant at the cervical or lumbar enlargements.
Sensory deficit. Destruction of the posterior column results in loss of position sense, vibration and tactile discrimination below the level of the lesion on the affected side. Destruction of the lateral spinothalamic tract causes loss of sensation of pain and temperature on the side opposite to the lesion. As the fibres entering this tract do not cross for several segments, the upper level of this sensory loss is likely to be a few segments below the level of the lesion.
Fibres entering the cord at the level of the lesion may be involved before they cross, causing a narrow zone of similar pain and temperature loss on the same side.
Typical cases of Brown-Sequard Syndrome are rare. Many patients with incomplete lesions will present with some asymmetry whilst not fulfilling the exact criteria of this syndrome.
Patients with a total severance of the lateral half of their spinal cord will have little if any recovery, whereas those with contusions or contracoup injuries are likely to show significant functional improvement.
The majority of these patients will walk independently, with a reciprocal gait, as only one leg has lost or reduced motor power. An orthosis and/ or walking aids may be required. Even among the three syndromes described above, there is considerable variability in the severity of neurological damage and thus in the functional outcome. Incomplete spinal cord damage resulting from other pathologies, such as tumours, inflammatory disease, cervical myelopathy and vascular disease, is often more diverse and the outcome even more unpredictable.
SCI Related Pages







Further Reading
- Brown-Séquard syndrome. From Wikipedia, the free encyclopedia
- Brown-Séquard syndrome. MedScape
- BROWN SÉQUARD SYNDROME. rarediseases.org
- Brown-Séquard syndrome. WebMD
- NINDS Brown-Sequard Syndrome Information Page
- Brown-Sequard Syndrome. Apparelyzed.com - Spinal Cord Injury Peer Support
Return from Brown Sequard Syndrome to Home Page
Return from Brown Sequard Syndrome to Neuro Rehab
Recent Articles
|
Author's Pick
Rating: 4.4 Votes: 252 |


 About Prodyut Das (PT, DPT) Physical Therapist at SMC, New York, USA. Former PT Winner Regional Health, South Dakota, Former HOD Physiotherapy & Fitness center @ NIMT Hospital, Greater Noida. Former PT ISIC Hospital. DPT ( Univ of Montana), MPT (neuro), MIAP, cert. manual therapist, Medical Neuroscience (USA). Licensed Physical Therapist in NY and Texas, USA. |
Connect with me- |
© Copyright physiotherapy-treatment.com since 2009 |